

By Aimee Delorey, Ph.D., and Mark Miller of Symphony Health
It comes as no surprise that big data is being used in all aspects of human life, from where we shop, how we listen to music, how we date and more. But in healthcare analytics, it’s more than just collecting data for the sake of marketing, it’s about understanding how we as doctors treat our patients based on their everyday life habits and goals for living a healthy lifestyle.
The problem and the solution
Large scale data systems, like CRMs may not always provide a holistic, 360-degree view of the patient. They provide limited or incomplete databases in which healthcare professionals have to fill in the blanks. Gaps in data provide significant barriers in understanding patient behavior. Thus, patients receive underwhelming care. According to a 2015 study from McKinsey & Company, 95% of patient data resides outside of the care management system.[1]
 Doctors need to be merging traditional data with new sources in order to identify behavior, attitudes and life circumstances. Getting to know our patient’s stress levels, job responsibilities, food and exercise routines, hours spent using technology, social lives and more with the data provided to us will help us provide individualized treatment and advice.
Doctors need to be merging traditional data with new sources in order to identify behavior, attitudes and life circumstances. Getting to know our patient’s stress levels, job responsibilities, food and exercise routines, hours spent using technology, social lives and more with the data provided to us will help us provide individualized treatment and advice.
A 2016 study by the SAS Institute merged third party consumer data with claims data to predict healthcare utilization risk and costs.[2] As a result, researchers were able to identify TV viewing patterns, mail-order buying habits (including mail-order prescriptions) and investments in stocks and bonds. The culmination of all this information arms doctors with predictive power in helping understand a patient’s risk for particular outcomes and the related cost.
Using data to invoke change
The earlier we can detect and give our patients a diagnosis, the better their outcome will be. With more comprehensive data and information which is critical to the patient’s journey, (family history, lifestyle and comorbid conditions like diabetes or anemia) can lead to earlier detection.
For example, a main symptom of congestive heart failure is fatigue, which is not always a telling symptom to the average patient. Most patients aren’t diagnosed with this disease until the later stages, meaning most have been living with the disease for some time before diagnosis and treatment.
However, with the help of data, a physician can triangulate their historical information with current signs and symptoms to identify heart disease at an earlier time. This is significant to a patient suffering from unrecognized heart disease who can have a materially improved quality of life with the help of early detection and appropriate treatment.
Conclusion
It’s critical that the healthcare industry, from practitioners to pharmaceutical companies, to look to new ways to understand patients that go beyond traditional data sources, (i.e. wearable technology and the cloud). A better understanding of patients through data will vastly improve diagnosis, earlier detection, more effective treatment, aftercare, prevention and quality of care.
References
[1] McKinsey
[2] Statish Garla, Albert Hopping, Rock Moaco, Sarah Rittman. What Do Your Consumer Habits Say About Your Health Risk? Using Third-Party Data to Predict Individual Health Risk and Costs; SAS Institute, 2016
About the Authors
 Aimee Delorey, Ph.D., senior director, Strategy & Research at Symphony Health, has spent nearly 20 years in analytics and consulting roles serving biotechnology, pharmaceutical and health plan clients. Her areas of expertise include CRM strategy, marketing effectiveness, predictive modeling, data visualization and customer journeys.
Aimee Delorey, Ph.D., senior director, Strategy & Research at Symphony Health, has spent nearly 20 years in analytics and consulting roles serving biotechnology, pharmaceutical and health plan clients. Her areas of expertise include CRM strategy, marketing effectiveness, predictive modeling, data visualization and customer journeys.
 As the leader of Symphony’s Audience and Media practice, Mark Miller's team is responsible for helping clients design, measure and optimize highly complicated media and marketing initiatives. He does this by leveraging Symphony’s unique data and analytic capabilities with an eye towards effective and nimble marketing execution. Mark is widely regarded as one of the foremost thinkers in customer experience design with a focus on groundbreaking solutions in the areas of brand planning, digital media and CRM execution.
As the leader of Symphony’s Audience and Media practice, Mark Miller's team is responsible for helping clients design, measure and optimize highly complicated media and marketing initiatives. He does this by leveraging Symphony’s unique data and analytic capabilities with an eye towards effective and nimble marketing execution. Mark is widely regarded as one of the foremost thinkers in customer experience design with a focus on groundbreaking solutions in the areas of brand planning, digital media and CRM execution.
Editor's Note: Join Mark as he copresents with Britta Cleveland, SVP of Research with Meredith, at our DTC Forum on TV & Print, discussing the impact print ads have on Rx sales conversions and overall Return On Ad Spend (ROAS). The 2017 DTC Forum on TV & Print will be held Oct 26th in NYC.





 For the last two years, we have conducted a revealing survey among women making healthcare decisions asking how much they trust the pharmaceutical industry – the WEST Survey on Pharma: Women’s Engagement, Satisfaction & Trust. This year, we also conducted the same survey among 300 men, the MENT Survey on Pharma: Men’s Engagement, Needs & Trust, again through our subsidiary Health Stories Project, an online community of people inspired to tell their health stories to help others to connect and learn.
For the last two years, we have conducted a revealing survey among women making healthcare decisions asking how much they trust the pharmaceutical industry – the WEST Survey on Pharma: Women’s Engagement, Satisfaction & Trust. This year, we also conducted the same survey among 300 men, the MENT Survey on Pharma: Men’s Engagement, Needs & Trust, again through our subsidiary Health Stories Project, an online community of people inspired to tell their health stories to help others to connect and learn.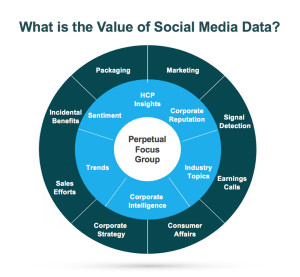 In the healthcare industry, patients and healthcare providers (HCPs) are looking to social media for information and support regarding their health and the health of their patients. They serve as a “perpetual focus group,” whose conversations taking place on social media provide brands with the opportunity to listen. Patients share their opinions, ask questions about diseases and treatment options, and directly or incidentally report adverse events. Meanwhile, HCPs voice opinions on the healthcare industry, provide thought leadership on a wide range of topics such as participatory medicine, reimbursement, and medical education. In a recent survey, more than 40 percent of respondents reported that information found via social media would affect the way they coped with a chronic condition or their approach to diet and exercise; 34 percent said it would affect taking certain medication.1 This demonstrates to companies that patients are directly impacted by what they view on social media and in order for brands to leverage that data radiating out of all the social conversations, several factors need to be in place.
In the healthcare industry, patients and healthcare providers (HCPs) are looking to social media for information and support regarding their health and the health of their patients. They serve as a “perpetual focus group,” whose conversations taking place on social media provide brands with the opportunity to listen. Patients share their opinions, ask questions about diseases and treatment options, and directly or incidentally report adverse events. Meanwhile, HCPs voice opinions on the healthcare industry, provide thought leadership on a wide range of topics such as participatory medicine, reimbursement, and medical education. In a recent survey, more than 40 percent of respondents reported that information found via social media would affect the way they coped with a chronic condition or their approach to diet and exercise; 34 percent said it would affect taking certain medication.1 This demonstrates to companies that patients are directly impacted by what they view on social media and in order for brands to leverage that data radiating out of all the social conversations, several factors need to be in place.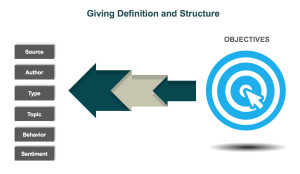 d is looking to identify who is talking about a product, the kinds of content they are posting, and the topics within their content, a structure that would classify posts into categories such as Consumer, Branded Product, and Medical Inquiry could be utilized. As more and more posts are tagged, patterns, trends, and themes can be identified.
d is looking to identify who is talking about a product, the kinds of content they are posting, and the topics within their content, a structure that would classify posts into categories such as Consumer, Branded Product, and Medical Inquiry could be utilized. As more and more posts are tagged, patterns, trends, and themes can be identified.

