

Specialty Drug Marketers Can Tap into Patient Stories
Stories are ingrained in us from the time we are infants. The nighttime ritual of parents and children cozying up with a storybook or two is a genuine and enjoyable encounter, one with an underlying message or lesson that is served in a palatable way. Once we begin reading for ourselves, we turn to stories to bring clarity to a topic, brighten an experience, or learn something new.
Patients often have many stories of their own to tell, no book needed. At each story’s core are kernels of information that can help biopharmaceutical marketers, healthcare professionals, and other patients understand an individual’s challenges and triumphs as well as reveal unmet needs and gaps in care.
What can be learned from the tale of an active female patient with rheumatoid arthritis? As it turns out, quite a lot. The story of Lisa Hehn’s journey includes a lot of twists and turns, revelations, and teaching moments relevant to brand marketers. Patient stories resonate. They illustrate real-life experiences, pull at heartstrings, and humanize disease.

Lisa’s Journey
Six months after her second child was born by cesarean section, Lisa woke up with total body pain. As a young mother, she needed to be well in order to care for her children and keep up with the daily demands of an active lifestyle that included walking, dance classes, and regular gym visits.
Lisa set out on an odyssey to discover the root cause of her pain and find a solution, relying primarily on library research and the expertise of numerous physicians and other healthcare professionals. Her pain was managed with anti-inflammatories, steroids, and other medications that left her with serious side effects including stomach bleeds. She wore wrist braces to carry her children, and even added carpet padding to her slippers to soften the pain of each step she took.
Years passed before a specialist diagnosed Lisa with rheumatoid arthritis and ultimately prescribed a TNF inhibitor to manage her disease. The change for Lisa was life-altering, in fact, she’s said that the biologic gave her life.
Drugstore Aisle Opportunities for Specialty Brands
Patient narratives like Lisa’s can help specialty brand marketers pinpoint effective marketing strategies across various channels at every step of the journey. Although Lisa’s disease is now well managed, that was not always the case. Prior to her diagnosis, she frequently shopped at the pharmacy for OTC solutions to address unidentified pain and other ailments related to an unknown disease.
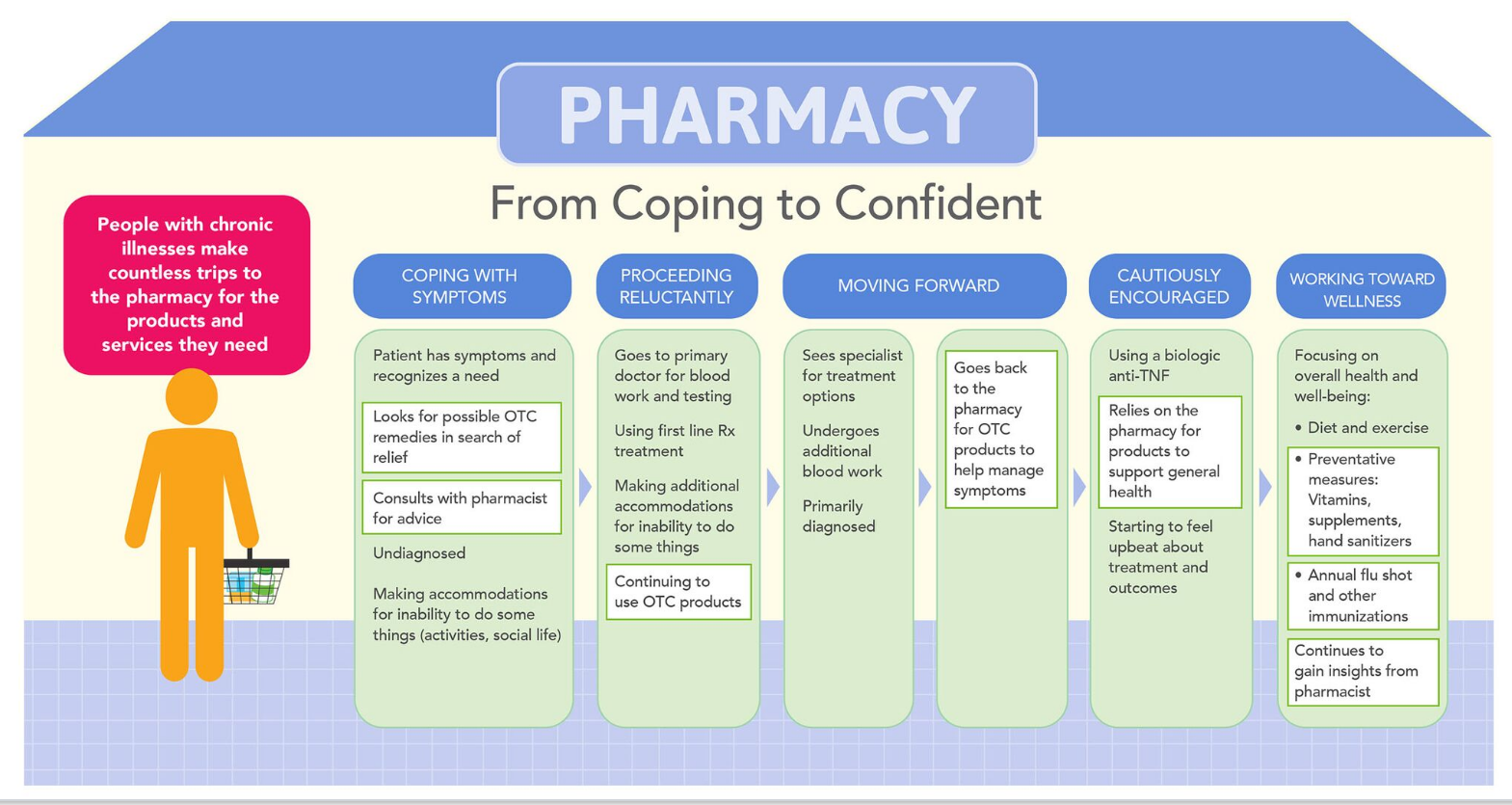
Once diagnosed with an autoimmune disease, prevention became a regular part of Lisa’s day. To minimize exposure to germs and viruses and thereby prevent illnesses, Lisa turned to the pharmacy for products including vitamins, over-the-counter pre-cold remedies, and hand sanitizers. In addition, as a mother, Lisa often shopped for health remedies and other products for her husband and children.
Patients gather information from various touchpoints and needs continue to evolve as a condition unfolds and treatments are prescribed. The pharmacy is a prime touchpoint because it’s a venue patients visit when they’re open to, and often seeking, health-related solutions and education.
At the beginning of the treatment continuum for a chronic disease such as RA, a patient may be most interested in the potential side effects of a particular therapy, whereas over time, concerns shift to more global issues including affordability and adherence.
Even now, Lisa seeks solutions for occasional health needs both related and unrelated to her main diagnosis. Though Lisa’s medication is filled through a specialty pharmacy and shipped to her home, she turns to retail and community pharmacies on a regular basis for a variety of needs.
Weaving the Pharmacy into a DTC Campaign
When handed a new diagnosis, and prescribed a new medication – whether traditional or specialty – patients often hunger for information, feedback, and guidance. Though each individual patient will seek information in different ways, knowledge is often gathered from multiple sources.
So how can the patient perspective help shape a DTC campaign? Listening to the patient experience can help brand marketers identify lingering needs and information gaps. In Lisa’s case, being prescribed a biologic nearly two decades ago left a lot of unanswered questions. She was starved for more information about RA but also how the biologic worked, how it would improve her symptoms, and what she could do to maximize its effect.
Though Lisa feels more medically savvy now out of necessity, at the time she would have liked access to educational content with patient-friendly language. To her, the pharmacy is well suited to disseminate simple messages about particular diseases and conditions.
When Lisa enters a pharmacy, she has health on her mind and she knows the onsite pharmacist is available to address questions and concerns. She finds the setting professional, comforting, and accessible for health-related messaging. In fact, if the option presented itself, she’d jump at the chance to pick up her specialty medication in the neighborhood pharmacy rather than receiving a shipment in her home.
Visiting the pharmacy is not a one-time event. Patients have different needs at each point along the way, affected by medication, age, and a variety of other factors. Patients with chronic diseases often continue to cope with a few minor symptoms, particularly at the beginning of a new treatment option. Therefore, the pharmacy can be a vehicle for driving patients to other resources such as a comprehensive disease website or online tools to help manage the disease burden.
Build Customer Awareness at the Pharmacy Level
With shrinking budgets and increased scrutiny of traditional DTC advertising, marketing tactics need to be more targeted, more effective, and less expensive. Specialty pharma marketers in particular are tasked with learning about the people taking their products, and that includes uncovering their needs. Who can clearly define patient needs and wants better than the patient himself?

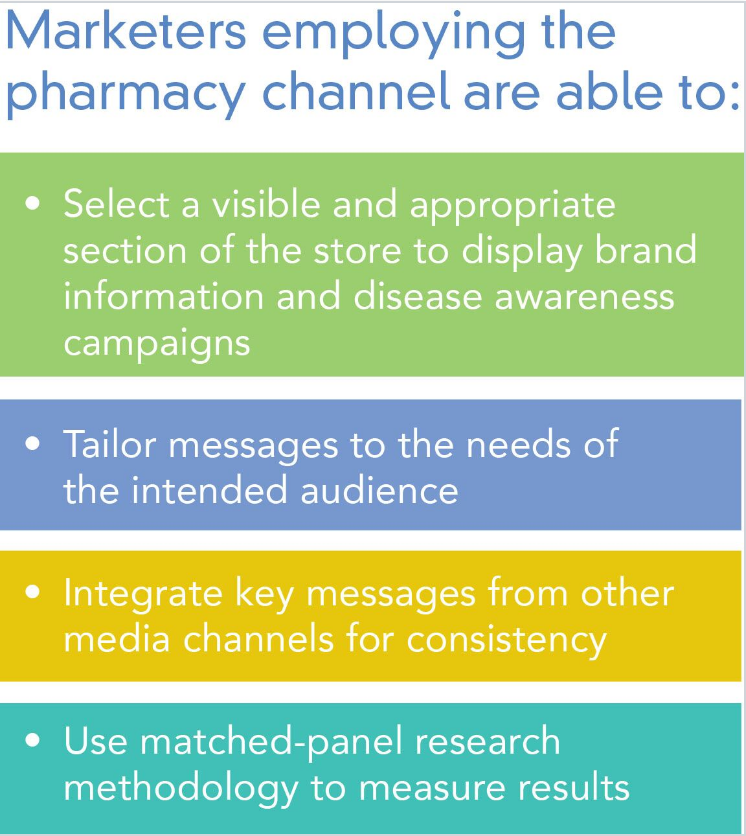
Listening to patients can help marketers identify the best messaging approach before creating a branded shelf aid in the pharmacy or creating a magazine advertisement. Targeted products for specific populations, like RA for example, require a targeted marketing plan even though the number of patients affected by the disease is large. In some cases, the patient pool prescribed specialty medications is quite small which requires a more focused messaging approach.
Patients rely on specialty pharmacies to dispense specialty medications; however, the same patients are also regularly stopping by retail pharmacies. In fact, these patients may spend even more time in drugstore aisles than the average consumer. It’s a moment in time when the patients have their own health concerns – and likely that of a child, parent, or spouse as well – top of mind.
The pharmacy is an appropriate setting to deliver strong messages to patients while they’re looking to improve their health. Drugstore aisles are a proven platform to reach patients with targeted and specific information that helps establish a close link and provide the support needed. In-store campaigns can also open the door to other media channels, driving the patient to continue the brand experience. Integrated programs that include multiple touchpoints such as mobile and internet reinforce messaging found in store aisles.
The Next Powerful Patient Story Awaits
Marketers hope the messages they develop motivate patients to take action. Some patients may respond positively to information about how a newly marketed product differs from those that have been available for years. Another patient type may want to be informed in order to open a conversation with a pharmacist or physician. The communication’s value and credibility increases exponentially by having a healthcare professional available in-store. Patients can easily discuss questions and concerns with a pharmacist and in some cases, a nurse practitioner or physician assistant.
We’ve all heard of the cardiologist who has an epiphany about what a patient truly needs once he himself has had to endure triple bypass surgery. When patients share real-life experiences of their diagnoses, it’s the closet way to feel their pain and see their struggle without actually having the disease ourselves. Keeping real-life patient stories in mind can elevate a marketing campaign’s effectiveness and ensure the product and patient develop a genuine and worthy connection.



