Changes in Patient Behaviors and Expectations Are Driving Shifts in Go-to-Market Strategies
The post-COVID era has normalized virtual healthcare, with telemedicine and home delivery now seen as standard expectations. Since 2022, most sources say that more than 30% of people used telemedicine services in the prior year, signaling a lasting shift toward digital-first care.
At the same time, there has been record-breaking e-commerce activity—such as Black Friday and Cyber Monday in 2024, where sales through Shopify hit a record $11.5B—reshaping consumer behavior. Trends like mobile and social shopping, along with buy-online-pickup-in-store (BOPIS) models, are influencing how patients expect to access medications. Compounding pharmacies and generic manufacturers have embraced these expectations, allowing patients to obtain many prescriptions through e-commerce-style experiences. Companies like Hims have demonstrated the power of this model, growing into a $7.5B business.
With the healthcare system stretched to capacity—especially in specialty care—virtual fulfillment offers a way to relieve pressure by streamlining access for patients who don’t require an in-person visit with a healthcare provider, allowing them to engage with a doctor via video or asynchronously via messaging. In response, over the past few years, many pharmaceutical brands have been launching white-labeled telemedicine and fulfillment platforms within brand.com to make treatment access faster and more convenient.
Larger manufacturers are scaling these efforts enterprise-wide: Eli Lilly introduced Lilly Direct in January 2024, and Pfizer launched PfizerForAll in August 2024; both platforms are designed to centralize patient education, support, and treatment information while giving patients greater control and clarity in how they obtain their medications.
While the initial DTP solutions have focused on lifestyle medications, driven by the GLP-1s, these solutions are poised to support treatments in areas that are low touch, and don’t really need specialist intervention. We’re starting to see that come to fruition, with solutions rolling out to support drugs in the asthma, lipid management, and migraine spaces.
Government and FDA Policy Shifts Are Accelerating the Rollout of Discounts and Direct-to-Patient (DTP) Solutions with Large Manufacturers
On May 12, 2025, the White House announced the Most-Favored-Nation Prescription Drug Price Presidential Action (MFN). MFN aims to reduce prescription drug prices and calls on the large pharmaceutical manufacturers to offer new ways for patients to access medications more affordably.
In June 2025, the FDA announced the Commissioner’s National Priority Voucher (CNPV) pilot program. This initiative, much like the existing FDA voucher program, grants accelerated approval for new drug launches. However, this new CNPV is only accessible to manufacturers “aligned with critical US national health priorities”—essentially incentivizing manufacturers to participate in MFN. This could change plans for in-market brands, as competitors may now launch sooner than originally planned—and at lower costs.
On September 29, 2025, PhRMA announced that it will support the White House’s programs, launching three actions that will deliver additional investments to the industry, provide further financial assistance to patients, and launch americasmedicines.com as a way to help patients access medications by consolidating DTP purchasing options for all medications and manufacturers. Shortly after, on September 30, the White House announced TrumpRx.gov, a website launching in January 2026, which allows patients to purchase medications as part of MFN directly.
From September through October 2025, the first partnerships under MFN have started to be announced, and it’s likely more will follow as the year continues:
- Partnership 1: Pfizer
- This partnership, announced on September 30, 2025, aims to bring Pfizer drugs to all state Medicaid programs at discounts of up to 80% when purchased directly
- Partnership 2: AstraZeneca (AZ)
- This partnership, announced on October 10, 2025, aims to bring AZ’s respiratory portfolio to all state Medicaid programs at discounts of up to 98% when purchased directly via AZPatientDirect.
- Partnership 3: EMD Serono
- This partnership, announced on October 16, 2025, aims to expand access to IVF and fertility treatments, and will bring EMD Serono’s fertility portfolio (Gonal-F, Ovidrel, and Certrotide) at deep discounts to those purchasing directly from TrumpRx.gov, starting in January 2026. Low- or middle-income women will be able to access further discounts.
While not announced by the White House, on September 25, BMS announced the launch of BMS Patient Connect, which will allow cash patients to receive Sotyktu at an 80% discount beginning in January 2026. This was a follow-up to their announcement of Eliquis 360 Support in July. On October 6, Amgen introduced AmgenNow, offering Repatha at a 60% discount off the list price to all patients.
On October 16, the FDA also communicated the recipients of the first wave of accelerated approvals under CNPV, which also included Pergoveris, EMD Serono’s fertility medication (currently approved in the EU and Canada), which will likely launch in January 2026.
We’re also starting to see the first partnerships that are connecting these online DTP platforms with traditional retail pharmacy—leveraging the trend toward BOPIS in consumer commerce. On October 29, Lilly announced a partnership with Walmart pharmacy, which is the first retail partnership that enables a pick-up option with direct-to-consumer pricing for Zepbound.
While these partnerships and announcements seem positive on the surface for lowering prices and enabling greater access to needed medications, they likely aren’t bringing price relief too broadly, and patients may have to jump through hoops to receive the discounted prices:
- Only available for cash-paying patients
- Only available for select government-insured patients with specific income requirements
- A requirement to bundle multiple medications together from the same manufacturer
- A requirement to purchase the medication from a specific third-party pharmacy
Additionally, there are clear underlying incentives for pharmaceutical companies to participate in MFN beyond driving greater access to medications. Partnering with the administration can:
- Get pipeline drugs considered for the CNPV program for accelerated drug approvals in 1–2 months
- Reduce or waive tariffs on pharmaceutical imports
Confusingly, many of these announcements around DTP pharmaceutical sales coincided with the tightening of the rules and regulations around DTC pharmaceutical advertising, with the wave of FDA Untitled Letters issued to manufacturers on September 9. This tightening of DTC promotion is somewhat incongruent with driving patients to obtain medications directly.
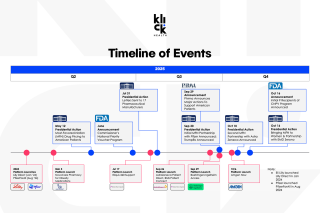
A Timeline of Key Events
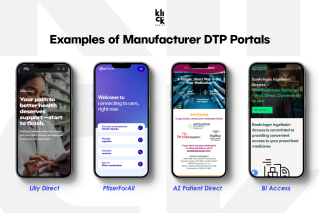
Examples of Manufacturer DTP Portals
What Does This Mean for Patients and Providers?
These changes have the potential to significantly improve how patients access their medications—making the process more convenient, flexible, and personalized. However, they also reshape the traditional role of the healthcare provider, introducing new dynamics in how care and fulfillment intersect.
Patients
For patients, these shifts can offer greater autonomy and control over their treatment experience. They may have more choices in how they pay for, receive, and manage their medications, which can enhance satisfaction and adherence. At the same time, the growing number of fulfillment options and support models may also create confusion. Patients may struggle to understand which programs apply to them, which are supported by their provider or insurer, and which option ultimately best serves their needs.
Additionally, as many of the discounted medications are only available under specific circumstances (e.g., for patients paying cash, those with specific government insurance, through a specific pharmacy, or bundled with other medications from that manufacturer), this could cause disappointment if patients don’t fully understand the offers.
Providers
For providers, these changes can bring both efficiency and complexity. On the positive side, a streamlined fulfillment process may free up time to focus on the patients who most need their expertise. However, as more manufacturers adopt unique DTP or hybrid distribution models, providers will need to adapt their workflows to manage incoming requests and coordinate with different pharmacies and platforms for fulfillment. Over time, this could even influence prescribing behavior—potentially fostering new forms of manufacturer loyalty based on ease of process, patient satisfaction, or administrative simplicity.
What Does This Mean for Marketers?
These shifts can create new opportunities for marketers, as regulatory precedents now support more customer-first branded solutions, and there are now more DTP capabilities that have become easier and faster to implement. However, there are also potential threats, especially for smaller biotechs, that must be carefully considered.
Opportunities
Virtual Fulfillment Experiences Are Now Table Stakes
Branded telehealth, fulfillment, and savings and support programs, once designed to address specific brand challenges, such as limited access or low coverage, are now becoming standard expectations. They must serve as a core component of a brand’s go-to-market strategy rather than a niche solution implemented for a specific need, but designing and implementing them through an impeccable customer experience is more important than ever.
Category Growth
In many therapeutic areas, expanded access options and manufacturer discounts may stimulate overall category growth. Patients who had previously discontinued treatment may re-enter the market to take advantage of these new solutions and reduced costs.
A More Holistic Brand Value Story & Broader Access
Historically, DTP efforts have focused on communicating co-pay support for commercially insured patients, often overlooking those without coverage or who would prefer to pay out of pocket. These new solutions allow brands to tell a more inclusive value story—one that addresses a broader range of patient needs, including discounted solutions for medicare/Medicaid patients—but doing so will require stronger internal and external alignment, particularly with managed markets teams. Additionally, these solutions may expand access to patients who are not in large metro areas or close to specialists
Threats
Risk of Patient Confusion and Switching
As the landscape continues to evolve, there’s a risk that satisfied patients may reconsider how or where they obtain their medication—or even switch to competitors offering these DTP solutions and/or discounts. It’s critical to clearly communicate that your brand remains easy to access, be transparent about cost and programs available, and to dispel any misconceptions that switching therapies offers an advantage. Brands should also be prepared to address patient questions about why certain DTP solutions and/or discounts are not currently part of their offering.
Unexpected Competitive Moves Eroding Market Share
- New DTP purchasing solutions or discounts for in-market brands drive share towards them
- As larger pharmaceutical companies form more partnerships, they may introduce new DTP solutions or drug discounts for in-market brands that could undercut direct competitors. For smaller biotechs, it’s essential to scenario plan—anticipating how these shifts could impact the business and preparing proactive messaging or alternative fulfillment strategies.
- Accelerated approvals for new brands bring new options to market, potentially stealing share
- Additionally, these partnerships for in-market brands may lead to accelerated approvals for new launches through the CNPV program. Brands should proactively monitor competitors’ pipelines, plan for the potential impact of early launches, and develop strategies to mitigate any resulting risks.
In Summary
Particularly for smaller biotechs, it’s valuable to establish a cross-functional DTP task force to proactively identify opportunities, anticipate risks, and monitor new announcements, partnerships, and launches. This task force should also evaluate the level of impact of any of these factors. In some cases, for example, where cash-pay volume is tiny, it may not actually equate to a large business impact.
As this space continues to evolve rapidly, staying nimble, agile, and prepared with a plan for likely scenarios will help minimize risk to your brand. We can help you proactively build a DTP strategy or competitive scenario plans to navigate this changing environment.